Pheochromocytoma
Chromaffin tumors; Paraganglionoma
Pheochromocytoma is a rare tumor of adrenal gland tissue that typically arises from the adrenal gland. It results in the release of too much epinephrine and norepinephrine, which are hormones that control heart rate, metabolism, and blood pressure.
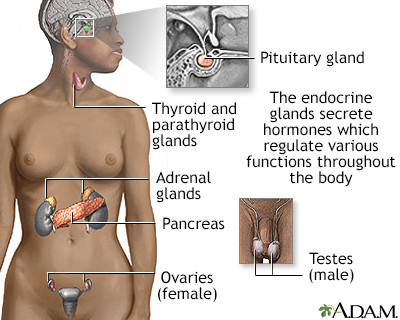
Endocrine glands release hormones (chemical messengers) into the bloodstream to be transported to various organs and tissues throughout the body. For instance, the pancreas secretes insulin, which allows the body to regulate levels of sugar in the blood. The thyroid gets instructions from the pituitary to secrete hormones which determine the rate of metabolism in the body (the more hormone in the bloodstream, the faster the chemical activity; the less hormone, the slower the activity).
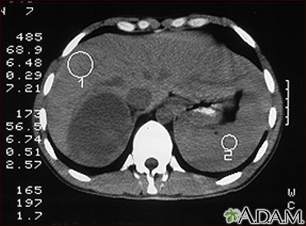
This CT scan of the upper abdomen shows an adrenal metastasis (spreading of a tumor to the adrenal gland, above the kidney) in a person with lung cancer.
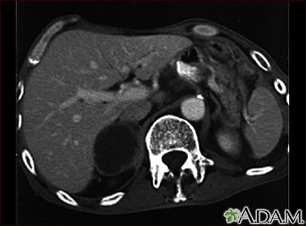
CT scan of the upper abdomen in a person with a right adrenal mass. The adrenal glands are located above the kidneys.
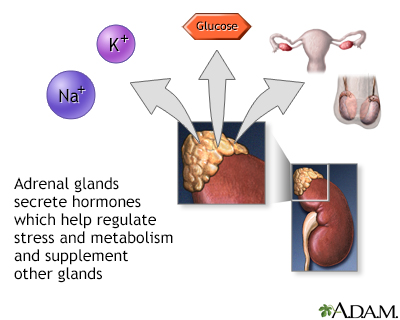
The adrenal gland secretes steroid hormones such as cortisol and aldosterone. It also makes precursors that can be converted to sex steroids (androgen, estrogen). A different part of the adrenal gland makes adrenaline (epinephrine). When the glands produce more or less hormones than required by the body, disease conditions may occur.
Causes
Pheochromocytoma may occur as a single tumor or as more than one growth. It usually develops in the center (medulla) of one or both adrenal glands. The adrenal glands are two triangle-shaped glands. One gland is located on top of each kidney. In rare cases, a pheochromocytoma occurs outside the adrenal gland. When it does, it is usually somewhere else in the abdomen.
Very few pheochromocytomas are cancerous.
The tumors may occur at any age, but they are most common from early to mid-adulthood.
In few instances, the condition may also be seen among family members (hereditary).
Symptoms
Most people with this tumor have attacks of a set of symptoms, which happen when the tumor releases hormones. The attacks usually last from a few minutes to hours. The set of symptoms include:
- Headaches
- Heart palpitations
- Sweating
- High blood pressure
As the tumor grows, the attacks often increase in frequency, length, and severity.
Other symptoms that may occur include:
- Abdominal or chest pain
- Irritability, nervousness
- Pallor
- Weight loss
- Nausea and vomiting
- Shortness of breath
- Seizures
- Problems sleeping
Exams and Tests
Your health care provider will perform a physical exam. You'll be asked about your medical history and symptoms.
Tests done may include:
- Abdominal CT scan
- Adrenal gland biopsy
- Catecholamines blood test (serum catecholamines)
- Glucose test
- Metanephrine blood test (serum metanephrine)
- An imaging test called an MIBG scintiscan
- MRI of abdomen
- Urine catecholamines
- Urine metanephrines
- PET scan of abdomen
- Bone scan
Treatment
Treatment involves removing the tumor with surgery. It is important to stabilize your blood pressure and pulse with certain medicines before surgery. You may need to stay in the hospital and have your vital signs closely monitored around the time of surgery. After surgery, your vital signs will be continuously monitored in an intensive care unit.
When the tumor cannot be surgically removed, you will need to take medicine to manage it. A combination of medicines is usually needed to control the effects of the extra hormones. Radiation therapy and chemotherapy won't cure this kind of tumor, but they may help control the disease and treat symptoms that arise.
Outlook (Prognosis)
Most people who have noncancerous tumors that are removed with surgery are still alive after 5 years. The tumors come back in some people. Levels of the hormones norepinephrine and epinephrine return to normal after surgery.
Continued high blood pressure may occur after surgery. Standard treatments can usually control the high blood pressure.
People who have been successfully treated for pheochromocytoma should have testing from time to time to make sure the tumor has not returned. Close family members may also benefit from testing, because some cases are inherited.
When to Contact a Medical Professional
Contact your provider if you:
- Have symptoms of pheochromocytoma, such as headache, sweating, and palpitations
- Had a pheochromocytoma in the past and your symptoms return
References
Cameron J. Endocrine glands. In: Cameron AM, Cameron JL, eds. Current Surgical Therapy. 14th ed. Philadelphia, PA: Elsevier; 2023:Sect 13, 809-894.
National Cancer Institute website. Pheochromocytoma and paraganglioma treatment (PDQ) - health professional version.
Pacak K, Timmers HJLM, Taieb D, Lenders JWM, Eisenhofer G. Pheochromocytoma. In: Robertson RP, Giudice LC, Grossman AB, Hammer GD, Jensen MD, Kahaly GJ, et al, eds. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 99.
Version Info
Last reviewed on: 7/29/2024
Reviewed by: Warren Brenner, MD, Oncologist, Lynn Cancer Institute, Boca Raton, FL. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 02/24/2025.
