Ureteral retrograde brush biopsy
Biopsy - brush - urinary tract; Retrograde ureteral brush biopsy cytology; Cytology - ureteral retrograde brush biopsy
Ureteral retrograde brush biopsy is a surgical procedure. During the surgery, your doctor (urologist) takes a small sample of tissue from the lining of the kidney or ureter. The ureter is the tube that connects a kidney to the bladder. The tissue is sent to a lab for testing.
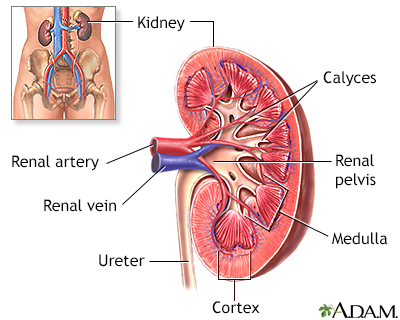
The kidneys are responsible for removing wastes from the body, regulating electrolyte balance and blood pressure, and the stimulation of red blood cell production.
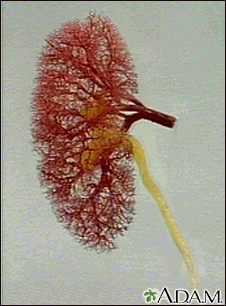
This is the typical appearance of the blood vessels (vasculature) and urine flow pattern in the kidney. The blood vessels are shown in red and the urine flow pattern in yellow.
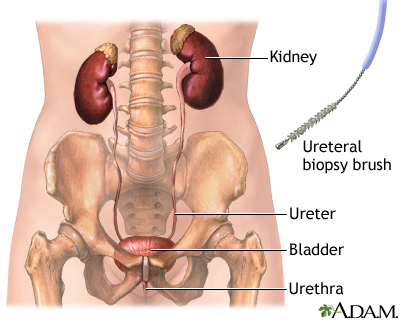
The cystoscope enters through the urethra, then the bladder, in order for the guidewire to gain access to the ureter.
How the Test is Performed
This procedure is done using:
- Regional (spinal) anesthesia
- General anesthesia
You will not feel any pain. The test takes about 30 to 60 minutes.
A cystoscope is first placed through the urethra into the bladder. A cystoscope is a tube with a camera on the end.
- Then a guide wire is inserted through the cystoscope into the ureter (the tube between the bladder and kidney).
- The cystoscope is removed. But the guide wire is left in place.
- A ureteroscope is inserted over or next to the guide wire. The ureteroscope is a longer, thinner telescope with a small camera. The surgeon can see the inside of the ureter or kidney through the camera.
- A nylon or steel brush is placed through the ureteroscope. The area to be biopsied is rubbed with the brush. Biopsy forceps may be used instead to collect a tissue sample.
- The brush or biopsy forceps is removed. The tissue is taken from the instrument.
The sample is then sent to a pathology lab for analysis. The instrument and guide wire are removed from the body. A small tube or stent may be left in the ureter. This prevents a kidney blockage caused by swelling from the procedure. It is removed later.
How to Prepare for the Test
You may not be able to eat or drink anything for about 6 hours before the test. Your health care provider will tell you how to prepare.
How the Test will Feel
You may have some mild cramping or discomfort after the test is over. You may have a burning feeling the first few times you empty your bladder. You may also urinate more often or have some blood in your urine for a few days after the procedure. You may have discomfort from the stent that will continue to be in place until it is removed at a later time.
Why the Test is Performed
This test is used to take a sample of tissue from the kidney or ureter. It is performed when an x-ray or other test has shown a suspicious area (lesion). This can also be done if there is blood or abnormal cells in the urine.
Normal Results
The tissue appears normal.
What Abnormal Results Mean
Risks
Risks for anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Bleeding, blood clots
- Infection
Another possible risk for this procedure is damage that creates a hole (perforation) in the ureter. This can cause scarring of the ureter and you may need another surgery to correct the problem. Tell your doctor if you have an allergy to seafood. This could cause you to have an allergic reaction to the contrast dye used during this test.
Considerations
This test should not be performed in people with a:
- Urinary tract infection
- Blockage at or below the biopsy site
You may have abdominal pain or pain on your side (flank).
A small amount of blood in the urine is normal the first few times you urinate after the procedure. Your urine may look faintly pink. Report very bloody urine or bleeding that lasts longer than 3 emptyings of the bladder to your doctor.
Contact your doctor if you have:
- Pain that is bad or is not getting better
- Fever
- Chills
- Very bloody urine
- Bleeding that continues after you have emptied your bladder 3 times
References
Kallidonis P, Liatsikos E. Urothelial tumors of the upper urinary tract and ureter. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 98.
National Institute of Diabetes and Digestive and Kidney Diseases website. Cystoscopy & ureteroscopy.
Version Info
Last reviewed on: 5/17/2024
Reviewed by: Sovrin M. Shah, MD, Associate Professor, Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
