Broken bone
Bone - broken; Fracture; Stress fracture; Bone fracture
If more pressure is put on a bone than it can stand, it will split or break. A break of any size is called a fracture. If the broken bone punctures the skin, it is called an open fracture (compound fracture).
A stress fracture is a break in the bone that develops because of repeated or prolonged forces against the bone. The repeated stress weakens the bone until it finally breaks.
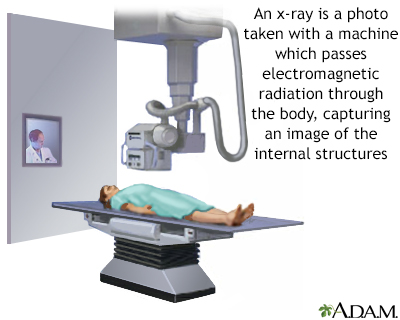
X-rays are a form of ionizing radiation that can penetrate the body to form an image on film. Structures that are dense (such as bone) will appear white, air will be black, and other structures will be shades of gray depending on density. X-rays can provide information about obstructions, tumors, and other diseases, especially when coupled with the use of barium and air contrast within the bowel.
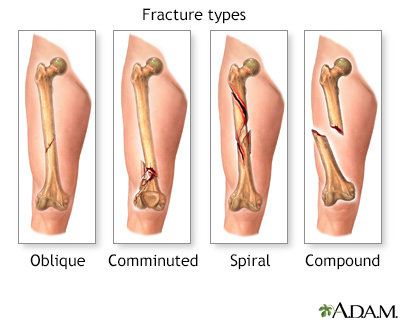
There are several types of bone fracture, including oblique -- a fracture which goes at an angle to the axis, comminuted -- a fracture of many relatively small fragments, spiral -- a fracture which runs around the axis of the bone, and compound -- a fracture (also called open) which breaks the skin.

This X-ray shows broken (fractured) forearm bones (radius and ulna).

This picture shows a normal osteoclast. It is a large cell with separately identifiable, multiple nuclei. Osteoclasts are needed to repair bone.
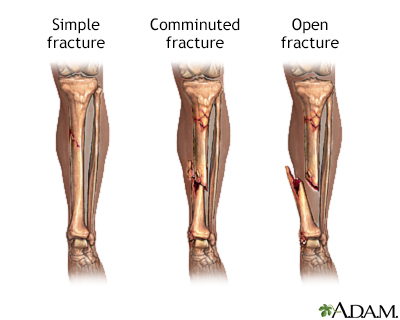
Fractures of the bones are classified in a number of ways. A simple fracture involves a single fracture line through a bone. A comminuted fracture is one in which the bone has been fractured into two or more fragments. An open fracture is one in which the fractured bone penetrates the skin.
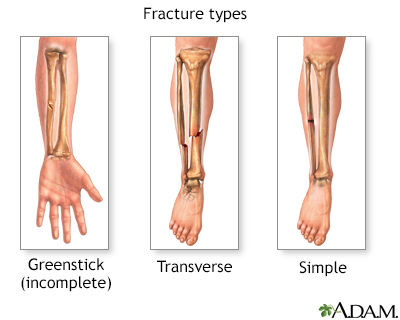
There are several types of bone fracture, including greenstick -- an incomplete fracture in which the bone bends, transverse -- a fracture that goes across the bones axis, and simple -- a fracture which does not break the skin.
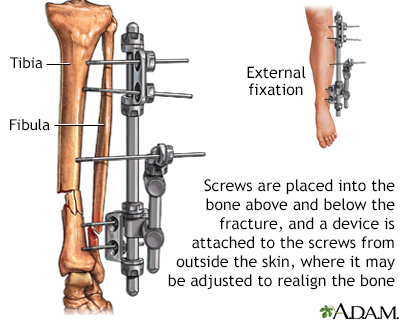
An external fixation device may be used to keep fractured bones stabilized and in alignment. The device can be adjusted externally to ensure the bones remain in an optimal position during the healing process. This device is commonly used in children and when the skin over the fracture has been damaged.
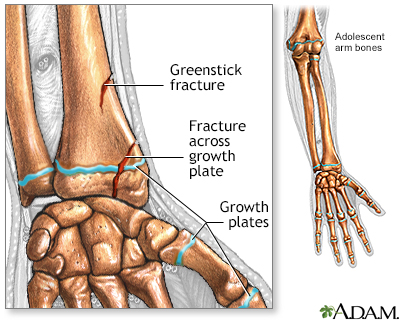
A green stick fracture is an incomplete fracture in a long bone of a child who has not finished growing. A fracture involving a growth plate (the cartilage plate near the end of the bone of a growing child where growth occurs) can lead to disturbances in growth of the bone, even if treated properly.
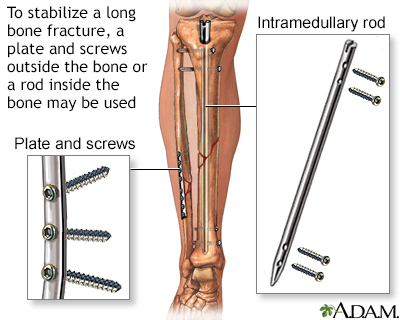
An internal fixation device may be used to keep fractured bones stabilized and in alignment. The device is inserted surgically to ensure the bones remain in an optimal position during and after the healing process.
Considerations
It may be hard to tell a dislocated joint from a broken bone. However, both are emergency situations, and the basic first aid steps are the same.
Causes
The following are common causes of broken bones:
- Fall from a height
- Trauma
- Motor vehicle accidents
- Direct blow
- Child abuse
- Repetitive forces, such as those caused by running, can cause stress fractures of the foot, ankle, tibia, or hip
Symptoms
Symptoms of a broken bone include:
- A visibly out-of-place or misshapen limb or joint
- Swelling, bruising, or bleeding
- Intense pain
- Numbness and tingling
- Broken skin with bone protruding
- Limited mobility or inability to move a limb or put weight on the leg
First Aid
First aid steps include:
- Check the person's airway and breathing. If necessary, call 911 or the local emergency number and begin rescue breathing, CPR, or bleeding control.
- Keep the person still and calm.
- Examine the person closely for other injuries.
- In most cases, if medical help responds quickly, allow the medical personnel to take further action.
- If the skin is broken, it should be treated right away to prevent infection. Call emergency help right away. DO NOT breathe on the wound or probe it. Try to cover the wound to avoid further contamination. Cover with sterile dressings if they are available. Don't try to line up the fracture unless you are medically trained to do so.
- If needed, immobilize the broken bone with a splint or sling. Possible splints include a rolled up newspaper or strips of wood. Immobilize the area both above and below the injured bone.
- Apply ice packs to reduce pain and swelling. Elevating the limb can also help to reduce swelling.
- Take steps to prevent shock. Lay the person flat, elevate the feet about 12 inches (30 centimeters) above the head, and cover the person with a coat or blanket. However, DO NOT move the person if a head, neck, or back injury is suspected.
CHECK BLOOD CIRCULATION
Check the person's blood circulation. Press firmly over the skin beyond the fracture site. (For example, if the fracture is in the leg, press on the foot). It should first blanch white and then "pink up" in about 2 seconds. Signs that circulation is inadequate include pale or blue skin, numbness or tingling, and loss of pulse.
If circulation is poor and trained personnel are NOT quickly available, try to realign the limb into a normal resting position. This will reduce swelling, pain, and damage to the tissues from lack of blood.
TREAT BLEEDING
Place a dry, clean cloth over the wound to dress it.
If the bleeding continues, apply direct pressure to the site of bleeding. DO NOT apply a tourniquet to the extremity to stop the bleeding unless it is life threatening. Tissue can only survive for a limited amount of time once a tourniquet is applied.
Do Not
- DO NOT move the person unless the broken bone is stable.
- DO NOT move a person with an injured hip, pelvis, or upper leg unless it is absolutely necessary. If you must move the person, pull the person to safety by their clothes (such as by the shoulders of a shirt, a belt, or pant legs).
- DO NOT move a person who has a possible spine injury.
- DO NOT attempt to straighten a bone or change its position unless blood circulation appears hampered and no medically trained personnel are nearby.
- DO NOT try to reposition a suspected spine injury.
- DO NOT test a bone's ability to move.
When to Contact a Medical Professional
Call 911 or the local emergency number if:
- The person is not responding or is losing consciousness.
- There is a suspected broken bone in the head, neck, or back.
- There is a suspected broken bone in the hip, pelvis, or upper leg.
- You cannot completely immobilize the injury at the scene by yourself.
- There is severe bleeding.
- An area below the injured joint is pale, cold, clammy, or blue.
- There is a bone projecting through the skin.
Even though other broken bones may not be medical emergencies, they still deserve medical attention. Contact your health care provider to find out where and when to be seen.
If a young child refuses to put weight on an arm or leg after an accident, won't move the arm or leg, or you can clearly see a deformity, assume the child has a broken bone and get medical help.
Prevention
Take the following steps to reduce your risk of a broken bone:
- Wear protective gear while skiing, biking, roller blading, and participating in contact sports. This includes using a helmet, elbow pads, knee pads, wrist guards, and shin pads.
- Create a safe home for young children. Place a gate at stairways and keep windows closed.
- Teach children how to be safe and look out for themselves.
- Supervise children carefully. There is no substitute for supervision, no matter how safe the environment or situation appears to be.
- Prevent falls by not standing on chairs, counter tops, or other unstable objects. Remove throw rugs and electrical cords from floor surfaces. Use handrails on staircases and non-skid mats in bathtubs. These steps are especially important for older people.
References
Geiderman JM, Torbati S. General principles of orthopedic injuries. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 41.
Kim C, Kaar SG. Commonly encountered fractures in sports medicine. In: Miller MD, Thompson SR, eds. DeLee Drez & Miller's Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 10.
Whittle AP. General principles of fracture treatment. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 53.
Version Info
Last reviewed on: 2/8/2024
Reviewed by: Linda J. Vorvick, MD, Clinical Professor, Department of Family Medicine, UW Medicine, School of Medicine, University of Washington, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
