Sodium blood test
Serum sodium; Sodium - serum
The sodium blood test measures the concentration of sodium in the blood.
Sodium can also be measured using a urine test.
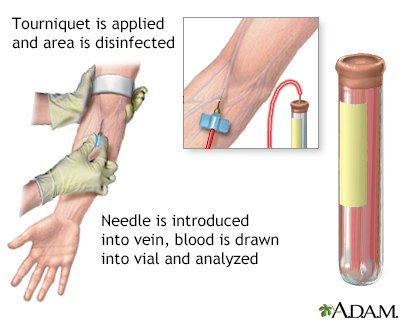
Blood is drawn from a vein (venipuncture), usually from the inside of the elbow or the back of the hand. A needle is inserted into the vein, and the blood is collected in an air-tight vial or a syringe. Preparation may vary depending on the specific test.
How the Test is Performed
A blood sample is needed.
How to Prepare for the Test
Your health care provider may tell you to temporarily stop taking medicines that may affect the test. These include:
- Antibiotics
- Antidepressants
- Some high blood pressure medicines
- Lithium
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Water pills (diuretics)
Do not stop taking any medicine without talking to your provider.
How the Test will Feel
When the needle is inserted to draw blood, some people feel moderate pain. Others feel only a prick or stinging. Afterward, there may be some throbbing or slight bruising. This soon goes away.
Why the Test is Performed
Sodium is a substance that the body needs to work properly. Sodium is found in most foods. The most common form of sodium is sodium chloride, which is table salt.
This test is usually done as part of an electrolyte or basic metabolic panel blood test.
Your blood sodium level represents a balance between the sodium and water in the food and drinks you consume and the amount in your urine. A small amount is lost through stool and sweat.
Many things can affect this balance. Your provider may order this test if you:
- Have had a recent injury, surgery, or serious illness
- Consume usually large or small amounts of salt or fluid
- Receive intravenous (IV) fluids
- Take diuretics (water pills) or certain other medicines, including the steroid hormones such as hydrocortisone
Normal Results
The normal range for blood sodium levels is 135 to 145 milliequivalents per liter (mEq/L).
Normal value ranges may vary slightly among different laboratories. Some labs use different measurements or test different samples. Talk to your provider about the meaning of your specific test results.
What Abnormal Results Mean
An abnormal sodium level can be due to many different conditions.
Higher than normal sodium level is called hypernatremia. It may be due to:
- Adrenal gland problems such as Cushing syndrome or hyperaldosteronism
- Diabetes insipidus (type of diabetes in which kidneys are not able to conserve water)
- Increased fluid loss due to excessive sweating, diarrhea, or burns
- Too much salt or sodium bicarbonate in the diet
- Use of certain medicines, including corticosteroids, laxatives, lithium, and medicines such as ibuprofen or naproxen
Lower than normal sodium level is called hyponatremia. It may be due to:
- Adrenal glands not making enough of their hormones (Addison disease)
- Buildup in urine of waste product from fat breakdown (ketonuria)
- High blood sugar level (hyperglycemia)
- High blood triglyceride lever (hypertriglyceridemia)
- Increase in total body water seen in those with heart failure, certain kidney diseases, or cirrhosis of the liver
- Increased fluid loss from body, vomiting, or diarrhea
- Syndrome of inappropriate antidiuretic hormone secretion (antidiuretic hormone is released in abnormal amounts or from an abnormal place in the body)
- Too much of the hormone vasopressin
- Underactive thyroid gland (hypothyroidism)
- Use of medicines such as diuretics (water pills), morphine, and selective serotonin reuptake inhibitor (SSRI) antidepressants
Risks
There is very little risk involved with having your blood taken. Veins and arteries vary in size from one person to another and from one side of the body to the other. Taking blood from some people may be more difficult than from others.
Other risks associated with having blood drawn are slight but may include:
- Excessive bleeding
- Multiple punctures to locate veins
- Fainting or feeling lightheaded
- Hematoma (blood accumulating under the skin)
- Infection (a slight risk any time the skin is broken)
References
Al-Awqati Q, Radhakrishnan J. Disorders of sodium and water. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 102.
Oh MS, Briefel G, Pincus MR. Evaluation of renal function, water, electrolytes, and acid-base balance. In: McPherson RA, Pincus MR, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods. 24th ed. Philadelphia, PA: Elsevier; 2022:chap 15.
Version Info
Last reviewed on: 11/20/2023
Reviewed by: Jacob Berman, MD, MPH, Clinical Assistant Professor of Medicine, Division of General Internal Medicine, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
