ACL reconstruction
Anterior cruciate ligament repair; Knee surgery - ACL; Knee arthroscopy - ACL
ACL reconstruction is surgery to reconstruct the ligament in the center of your knee. The anterior cruciate ligament (ACL) connects your shin bone (tibia) to your thigh bone (femur). A tear of this ligament can cause your knee to give way during physical activity, most often during side-step or crossover movements.
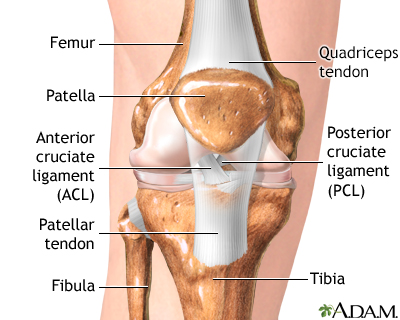
The anterior cruciate ligament (ACL) is a ligament in the center of the knee that prevents the shin bone (tibia) from moving forward on the thigh bone (femur).
Description
Most people have general anesthesia right before surgery. This means you will be asleep and pain-free. Other kinds of anesthesia, like regional anesthesia or a block, may also be used for this surgery.
The tissue to replace your damaged ACL will come from your own body or from a donor. A donor is a person who has died and chose to give all or part of their body to help others.
- Tissue taken from your own body is called an autograft. The most common places to take tissue from are the knee cap tendon, quadriceps tendon, or hamstring tendon. Your hamstrings are the muscles behind your knee.
- Tissue taken from a donor is called an allograft or cadaver graft.
The procedure is usually performed with the help of knee arthroscopy. With arthroscopy, a tiny camera is inserted into the knee through a small surgical cut. The camera is connected to a video monitor in the operating room. Your surgeon will use the camera to check the ligaments and other tissues of your knee.
Your surgeon will make other small cuts around your knee and insert other medical instruments. Your surgeon will fix any other damage found, and then will replace your ACL by following these steps:
- The torn ligament will be removed with a shaver or other instruments.
- If your own tissue is being used to make your new ACL, your surgeon will make a larger cut. Then, the autograft will be removed through this cut.
- Your surgeon will make tunnels and sockets in your bone through which to bring the new tissue. This new tissue will be put at the same place as your old ACL.
- Your surgeon will attach the new ligament to the bone with screws or other devices to hold it in place. As it heals, the graft will remodel to become your new ligament.
At the end of the surgery, your surgeon will close your cuts with sutures (stitches) and cover the area with a dressing. You may be able to view pictures after the procedure of what the surgeon saw and what was done during the surgery.
Why the Procedure Is Performed
If you do not have your ACL reconstructed, your knee may continue to be unstable. This increases the chance you may have a meniscus tear. ACL reconstruction may be used for these knee problems:
- Knee that gives way or feels unstable during daily activities
- Knee pain
- Inability to return to sports or other activities
- When other ligaments are also injured
- When your meniscus is torn
Before surgery, talk to your health care provider about the time and effort you will need to recover. You will need to follow a rehabilitation program for 4 to 6 months. Your ability to return to full activity will depend on how well you follow the program.
Risks
The risks from any anesthesia are:
- Allergic reactions to medicines
- Breathing problems
The risks from any surgery are:
- Bleeding
- Infection
Other risks from this surgery may include:
- Blood clot in the leg
- Failure of the ligament to heal
- Failure of the surgery to relieve symptoms
- Injury to a nearby blood vessel
- Pain in the knee
- Stiffness of the knee or lost range of motion
- Weakness of the knee
Before the Procedure
Always tell your provider what medicines you are taking, even medicines, supplements, or herbs you bought without a prescription.
During the 2 weeks before your surgery:
- You may be asked to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Naprosyn, Aleve), and other medicines.
- Ask your provider which medicines you should still take on the day of your surgery.
- If you have diabetes, heart disease, or other medical conditions, your surgeon will ask you to see the provider who treats you for these conditions.
- Tell your provider if you have been drinking a lot of alcohol, more than 1 drink per day for women or 2 drinks per day for men.
- If you smoke, try to stop. Smoking can slow down wound and bone healing. Ask your providers for help if you need it.
- Always let your provider know about any cold, flu, fever, herpes breakout, or other illnesses you may have before your surgery.
On the day of your surgery:
- You will often be asked not to drink or eat anything for 6 to 12 hours before the procedure.
- Take the medicines you have been told to take with a small sip of water.
- You will be told when to arrive at the hospital.
After the Procedure
Most people can go home the day of the surgery. You may have to wear a knee brace for the first 1 to 6 weeks. You also may need crutches for 1 to 6 weeks. How long you will need to use a crutch and brace will depend on the type of surgery you had and the extent of the reconstruction. Most people are allowed to move their knee right after surgery. This may help prevent stiffness. You may need medicine for your pain.
Physical therapy can help many people regain motion and strength in their knee. Therapy can last up to 4 to 6 months.
How soon you return to work will depend on the kind of work you do. It can be from a few days to a few months. A full return to activities and sports will often take 4 to 6 months. Sports that involve quick changes in direction, such as soccer, basketball, and football, may require up to 9 to 12 months of rehabilitation.
Outlook (Prognosis)
Most people will have a stable knee that does not give way after ACL reconstruction. Better surgical methods and rehabilitation have led to:
- Less pain and stiffness after surgery
- Fewer complications with the surgery itself
- Faster recovery time
References
Brotzman SB. Anterior cruciate ligament injuries. In: Giangarra CE, Manske RC, eds. Clinical Orthopaedic Rehabilitation: A Team Approach. 4th ed. Philadelphia, PA: Elsevier; 2018:chap 47.
Cheung EC, McAllister DR, Petrigliano FA. Anterior cruciate ligament injuries. In: Miller MD, Thompson SR, eds. DeLee, Drez, & Miller's Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 98.
Noyes FR, Barber-Westin SD. Anterior cruciate ligament primary reconstruction: diagnosis, operative techniques, and clinical outcomes. In: Noyes FR, Barber-Westin SD, eds. Noyes' Knee Disorders Surgery, Rehabilitation, Clinical Outcomes. 2nd ed. Philadelphia, PA: Elsevier; 2017:chap 7.
Phillips BB, Mihalko MJ. Arthroscopy of the lower extremity. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 40.
Version Info
Version: 2.0
Last reviewed on: 4/24/2023
Reviewed by: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
